





The ideal time to address a progressing idiopathic scoliosis curve is typically before the adolescent growth spurt, a period when the curve is likely to worsen rapidly. Current medical guidelines often recommend using a rigid back brace during this critical phase to reduce the risk of severe spinal deformity.
When to Consider Bracing
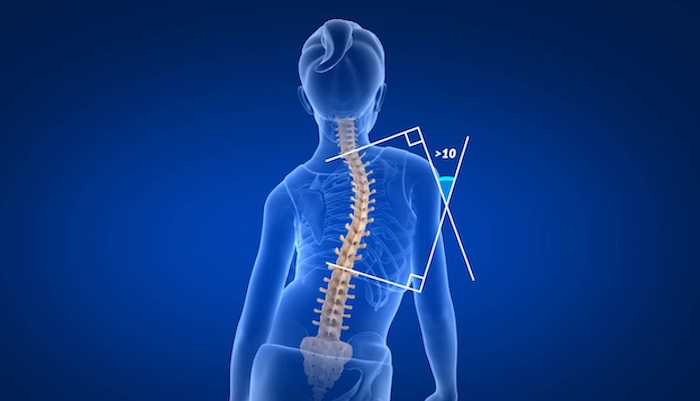
Scoliosis is defined as any sideways curvature of the spine measuring at least 10 degrees based on the Cobb angle, determined through an x-ray. When the Cobb angle is between 10 and 25 degrees, the usual approach is careful observation. This involves taking x-rays every 4 to 6 months to monitor any curve progression.
Bracing is typically recommended if one of the following criteria is met:
- The Cobb angle reaches at least 25 degrees, and the adolescent still has significant growth remaining.
- The Cobb angle is under 25 degrees but has increased by at least 5 degrees within a 4- to 6-month period.
If an adolescent is nearing full skeletal maturity, bracing is unlikely to be recommended as it is less effective at that stage.
Purpose of Bracing
While scoliosis curves rarely improve without surgery, research shows that wearing a brace as instructed can often prevent further curve progression. This makes bracing a useful method for keeping the curve small and manageable.
If a scoliosis curve reaches 50 degrees by skeletal maturity (usually around 14-15 years for girls and 16-17 years for boys), it will likely worsen into adulthood. Such severe curves typically require surgical intervention. Therefore, the primary goal of bracing is to avoid the need for major surgery by either halting curve progression or preventing it from reaching 40-50 degrees by maturity.
How Bracing Works
Braces apply corrective pressure to shift load away from the inner (concave) side of the curve and onto the outer (convex) side. The aim is to slow growth on the side that needs less growth and potentially increase it on the side that needs more. Although bracing does not usually reverse a curve, it can significantly slow or stabilize its progression until the child reaches skeletal maturity, at which point the curve is less likely to worsen if it remains under 40 degrees.
While the exact mechanisms behind bracing are still under study, current knowledge suggests that rigid braces are most effective due to the consistent pressure they apply.
Advances in Bracing
The Milwaukee brace, first developed in the 1940s, was an early innovation in scoliosis treatment. However, it was bulky, featured metal bars extending to the neck, and drew unwanted attention—particularly for teenagers. Compliance was low since few patients could tolerate wearing it for 23 hours daily.
By the 1970s and 80s, newer brace options emerged, including:
- Thoraco-lumbo-sacral orthosis (TLSO): This low-profile brace starts beneath the shoulders and can be worn discreetly under loose-fitting clothes, as it lacks metal bars or a neck component.
- Nighttime brace: Designed to apply stronger corrective forces while sleeping, this brace compensates for not being worn during the day. Since it’s only used while lying down, it doesn’t need counterbalances to align the head, allowing for greater pressure on the curve.
Precision Pain Care and Rehabilitation has two convenient locations in Richmond Hill – Queens, and New Hyde Park – Long Island. Call the Queens office at (718) 215-1888 or (516) 419-4480 for the Long Island office to arrange an appointment with our Interventional Pain Management Specialists, Dr. Jeffrey Chacko or Dr. Sonny Ahluwalia.





